

Prolonged repetitive throwing motions such as those familiar to baseball pitchers are a risk for developing repetitive strain injuries to the muscles, ligaments, and tendons supporting the inside of the elbow. These injuries are also common in athletes participating in overhead activities like tennis, badminton, and javelin throwing. The main symptom of this so-called “pitcher’s elbow” is a gradual onset of pain on the inside of the elbow that may travel down the inside of the forearm. Such high-velocity throwing motions place a lot of strain on the structures on the inside of the elbow, leading to microtears and possibly to the development of a repetitive strain injury. Ongoing sport participation without proper treatment may lead to an increase in the severity of the elbow pain, elbow swelling, and eventually decreased performance, like a slower fastball or a compromised tennis serve. This injury is known as medial epicondylitis. Prolonged injury without treatment may lead to an inability to compete.
Understanding which muscles, tendons, and ligaments are contracting, being pre-stretched, or are stabilizing the elbow joint in each of the five phases will help in developing a proper treatment and prevention program for medial epicondylitis.
Evaluation of the Pitching Motion
An effective pitching delivery (or overhead serve) involves rotation of the hips and torso in coordination with movement of the shoulder, elbow, and wrist. Two very successful professional pitchers, Nolan Ryan and Roger Clemens, were able to pitch effectively and relatively injury-free during their careers due to their regimented strength and conditioning programs and proper pitching mechanics. On the other hand, many pitchers with great arm strength but poor biomechanics have seen a premature end to their careers due to shoulder and elbow injuries. This article will focus on the biomechanics of pitching and stress placed on the elbow joint, which may lead to the development of medial epicondylitis.
There are 5 main pitching phases: the wind-up phase, stride/cocking phase, acceleration 1 phase, acceleration 2 phase, and follow-through phase (Figs. 1A-1H).
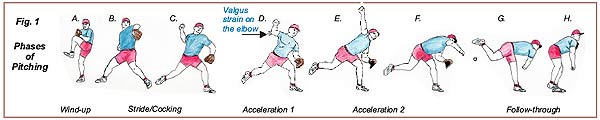
During the wind-up phase (Fig. 1A), the opposite knee of the pitching hand (the stride leg) is lifted to about waist level, the torso is extended slightly, and the hips are rotated towards the batter. The main purpose of the wind-up is to generate energy that will be transferred from the hips and torso to the arm during the later phases of throwing. Another purpose of the wind-up is to hide the style of pitch from the batter before it is delivered to the plate.
During the stride/cocking phase (Figs 1B-C), the pitching arm extends behind the head as the hand goes down, back, and up into the cocked position. Also during this phase the stride leg moves down and forward and the foot lands flatly on the ground. This pitching phase prepares the body to transfer the stored energy from the hips and torso to the shoulder and arm.
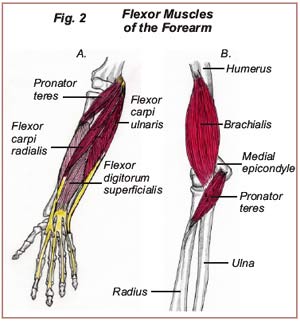
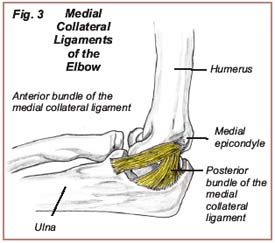
During the acceleration 1 phase (Fig. 1D), the body rotates towards home plate over the stride leg as the pitcher’s chest and shoulder come forward. The pitching arm is placed in extreme external rotation and there as an increased “valgus strain” placed on the structures supporting the inside of the elbow. Stabilization of the elbow joint during the acceleration 1 phase is dependent on the integrity of the muscles surrounding the elbow joint (Figs. 2A-B) and of the medial collateral ligaments, located on the inside of the elbow (Fig. 3). Injury to the medial collateral ligament will decrease performance and cause pain on the inside of the elbow. If this problem goes untreated, further tearing of the ligament may occur, possibly necessitating surgery to correct the problem.
 The power of the pitch is transferred from the torso and lower trunk to the shoulder, arm, and hand during acceleration 2 (Figs. 1E-F). During this phase, the trunk springs from extension (stretching out) to flexion (bending in) and rotates towards home plate over the planted stride leg. At the same time, the shoulder rotates internally and the arm and hand accelerate towards the plate until the baseball is released from the hand.
The power of the pitch is transferred from the torso and lower trunk to the shoulder, arm, and hand during acceleration 2 (Figs. 1E-F). During this phase, the trunk springs from extension (stretching out) to flexion (bending in) and rotates towards home plate over the planted stride leg. At the same time, the shoulder rotates internally and the arm and hand accelerate towards the plate until the baseball is released from the hand.
The follow-through phase (Figs. 1G-H) is the last phase of pitching and involves deceleration of the arm and hand after the baseball is released. The pitching arm, elbow, and hand should go down, over, and outside the lead leg while the other leg swings forward in line with the stride leg. The purpose of the follow-through is two-fold: arm deceleration (where the legs and back muscles aid the muscles, ligaments, and tendons of the shoulder, elbow, and arm); and preparation (placing the pitcher in a fielding position ready to field a ball hit in his direction).
 During the cocking and acceleration 1 phases, the wrist is slightly extended, stretching the flexor muscles of the forearm-the flexor digitorum superficialis, flexor carpi radialis, and flexor carpi ulnaris (Fig. 2A)-and an increased “valgus strain” is placed on the medial collateral ligament. From acceleration 1 to acceleration 2, the wrist goes from a slightly extended position to a flexed position, causing a forceful contraction of the forearm flexors. The tendons attached to these forearm flexors have a common insertion point on the medial epicondyle, an outgrowth of bone found on the inside and bottom of the humerus (arm bone). When these muscles are under-prepared and stretched in this way, tension develops in the tendons at the insertion point on the medial epicondyle. Overuse may cause microtears in these structures, causing pain at the medial epicondyle in the elbow.
During the cocking and acceleration 1 phases, the wrist is slightly extended, stretching the flexor muscles of the forearm-the flexor digitorum superficialis, flexor carpi radialis, and flexor carpi ulnaris (Fig. 2A)-and an increased “valgus strain” is placed on the medial collateral ligament. From acceleration 1 to acceleration 2, the wrist goes from a slightly extended position to a flexed position, causing a forceful contraction of the forearm flexors. The tendons attached to these forearm flexors have a common insertion point on the medial epicondyle, an outgrowth of bone found on the inside and bottom of the humerus (arm bone). When these muscles are under-prepared and stretched in this way, tension develops in the tendons at the insertion point on the medial epicondyle. Overuse may cause microtears in these structures, causing pain at the medial epicondyle in the elbow.
Improper pitching technique, including failure to utilize the trunk and torso effectively during the pitching phases, will place an increased workload onto the muscles, tendons, and ligaments of the arm, forearm, and hand, leading to overuse injuries. If the athlete does not improve pitching technique and/or fails to treat the condition appropriately, further injury will ensue, leading to the development of medial epicondylitis.
The overhead tennis or badminton swing would be similar to the cocking and acceleration 2 phases of the pitching motion. These athletes would benefit from exercises similar to those recommended for baseball pitchers.
Treatment and Prevention of Medial Epicondylitis/ Pitcher’s Elbow
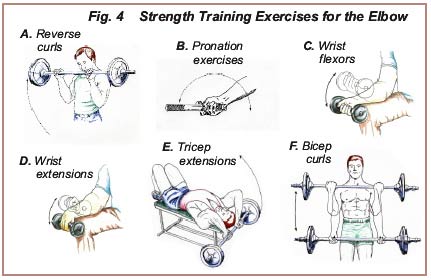
Repetitive strain injuries in the elbow region are directly related to the strength of the muscles as compared to the force acting on the muscles, and also to the number of repetitions performed. Strength training exercises consisting of reverse curls, pronation exercises, wrist flexors, wrist extensions, tricep extensions, and bicep curls (Figs. 4A-4F) will increase the strength of the muscles surrounding the elbow, allowing them to sustain more tension before injury. Such exercises also decrease the strain sustained by the medial collateral ligament during the pitching phases. Strength and flexibility training of the shoulder, abdominal, and leg muscles should also be included. Consult with a doctor before starting these exercises.
Off-season and pre-season conditioning should include pitching technique drills focusing on balance during the leg kick, proper stride technique, and coordinated hip rotation/trunk flexion combined with shoulder, arm and hand movements. A pitch count should be planned, limiting the number of pitches thrown until a base is established, and the velocity of the pitches should be increased at an appropriate rate during practice and pre-season games. After pitching, ice should be applied to the shoulder and elbow immediately, or as soon as possible, to decrease inflammation. After strenuous outings or workouts, an experienced sports therapist should be consulted to help relax the musculature surrounding the shoulder and elbow to assist in the prevention of injury.
Treatment of Pitcher’s Elbow at Dr. Dubin’s office would consist of:
- Deep tissue procedures to the muscles surrounding the shoulder, arm, and forearm to free up soft tissue motion
- Chiropractic adjustments of the wrist and elbow joints to free up joint motion
- Ultrasound and electric muscle stimulation combotherapy applied to the structures on the inside of the elbow to restore normal muscle tone, decrease pain, and absorb scar tissue
- Implementation of a personalized home strength program (Figs. 4A-4F), noting the importance of increasing strength and flexibility of the trunk musculature and the shoulder musculature
- Ice therapy applied to the elbow, 20 minutes on and one hour off after competition
- Recommendation to meet with a pro to improve pitching or swing technique.
Note: Consult with a doctor or certified strength conditioning specialist before starting these exercises.